Dr Bhavya
80year old with fever ,burning micturition and dysphagia
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box is welcome."I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan
80 year old female presented with the complains of fever since 3 months,
burning micturition since 3 months,
difficulty in swallowing since 1 month
HISTORY OF PRESENT ILLNESS
Patient was apparently assymptomatic 3 months back then developed fever associated with burning micturition & abdominal pain for which she was brought to the hospital and was admitted (pyrexia of unknown origin) and was discharged on 25/10/22 post which she had no complaints till 19/11/22 , when patient had similar complaints and was treated at local hospital
Previous record of hospital administration of patient
https://nehareddygaddam.blogspot.com/2022/10/72-female-with-fever-burning.html?m=1
On 10/12/22 patient presented to our hospital with complaints of fever since 20 days associated with burning micturition
Fever is low grade and continuous associated with chills & rigors , relieved partially with medication
K/c/o DM :20years on TAB.cinod T
HTN :on Inj.HAI 8u-x-6u
Surgery: Right PFN 11yrs ago
PERSONAL HISTORY:
Decreased appetite takes mixed diet, irregular bowels( Type 1 Bristol stool) ,normal micturition , no allergies
MENSTRUAL HISTORY:
Age of menarche - 15yrs
Menopause attained 30 years back
OBSTETRIC HISTORY:
Age at marriage-12yrs
Gravida 3 (all 3 are Full term NVD)
1st male , 2nd female - died
3rd - female alive
GENERAL PHYSICAL EXAMINATION
Patient conscious coherent cooperative
Moderately built and nourished
Pallor present

No, icterus, cyanosis, clubbing, lymphadenopathy
Vitals
Bp:150/90mmhg
RR-20cpm
PR-98bpm
SPO2-94%
GRBS-343mg/dl (inj. HAI 14 units given)
TEMP-98.3F
SYSTEMIC EXAMINATION :
RESPIRATORY SYSTEM EXAMINATION-
Inspection
Drooping of right shoulder
No engorged veins , discharging sinuses , scars
Apex beat cannot be seen
Trachea appears to be central
Palpation
Inspectory findings are confirmed
Trachea central
Decreased movements on right side
Vocal fremitus more on right side
Tactile fremitus more on right side
Percussion
Dull note on right side
Auscultation
Inspiratory crepts in the right inframammary area
Rest of the lung fields normal vesicular breath sounds
CVS: S1 , S2 present
Pansystolic murmur present
CNS: NAD
P/A: SOFT, TENDER
PROVISIONAL DIAGNOSIS:
PYREXIA OF UNKNOWN ORIGIN WITH ? PULM TB (ON ATT) ? CLINICAL MALARIA WITH HTN SINCE 20 YRS , TYPE II DM SINCE 20 YRS WITH ANAEMIA (NORMOCYTIC NORMOCHROMIC) WITH CHOLELITHIASIS
INVESTIGATIONS:
REPORTS-

Fever chart

2D Echo

ECG

Bacteria and culture sensitivity

USC Abdomen


USG Neck

X ray Neck


Chest x ray

HRCT Chest

HRCT CHEST Report



REFERRALS:
CARDIOLOGY REFERRAL

Surgery referral


ENT referral



PULMONOLOGY Referral

DVL referral


TREATMENT:
10/12/22
Patient presented with complaint of fever since 3 months on and off, difficulty in swallowing since 1 month
S
Fever
O
Pt is C/C/C
BP:110/70mmHg
PR:82bpm
RR:24cpm
SpO2:95% on RA
Temp :101 F
CVS:S1S2 +
RS :BAE +
PA-soft no organomegaly
A
PYREXIA UNDER EVALUATION
P
INJ. PIPTAZ 2.25 GM IV TID D7
INJ DOXY 100MG IV BD
INJ PAN 40MG IV OD
INJ NEOMOL 1GM IV SOS
TAB. DOLO 650 MG PO/TID
Vitals monitoring 4th hrly
GRBS monitoring 6th hrly
11/12/22
Patient presented with complaint of fever since 3 months on and off, difficulty in swallowing since 1 month
S
2 fever spikes @ 2:00 pm- 101f
@10pm - 102f
P
INJ. PIPTAZ 2.25 GM IV TID D7
INJ DOXY 100MG IV BD
INJ PAN 40MG IV OD
INJ NEOMOL 1GM IV SOS
TAB. ATT 3 TABLETS /DAY
TAB. CINOD T PO/OD
INJ. HAI ACCORDING TO GRBS- S/C
TAB. BENADON 40 MG PO/OD
INJ.FALCIGO 120mg IV/0th hr-12th hr-24th hr-48th hr
Tab NICARDIA 10mg PO/OD
Vitals monitoring 4th hrly
GRBS monitoring 6th hrly
13/12/22
Patient presented with complaint of fever since 3 months on and off, difficulty in swallowing since 1 month
S
1fever spike at 8:00 am- 101f and difficulty in swallowing
O
Pt is C/C/C
BP:160/90mmHg
PR:76bpm
RR:26cpm
SpO2:95% on RA
Temp :afebrile
CVS:S1S2 +
RS :BAE +
PA-soft no organomegaly
Temp :afebrile
CVS:S1S2 +
RS :BAE +
PA-soft no organomegaly
A
PYREXIA OF UNKNOWN ORIGIN WITH ? PULM TB ? CLINICAL MALARIA WITH HTN SINCE 20 YRS , TYPE II DM SINCE 20 YRS WITH ANAEMIA SECONDARY TO BLOOD LOSS OR NUTRITIONAL WITH CHRONIC CONSTIPATION(NORMOCYTIC NORMOCHROMIC) WITH CHOLELITHIASIS
P
TAB CINOD PO/BD
TAB MET- XL 25 MG PO/OD
TAB NICARDIA 10mg PO/SOS
TAB ULTRACET 1/2 tab PO/QID
Vitals monitoring 4th hrly
GRBS monitoring 6th hrly
Plan for HRCT and to withhold ATT today
18/12/22
P
TAB TELMA 40mg PO/OD
TAB METXL 25mg PO/OD
TAB AMLONG 5mg PO/OD
TAB NICARDIA 10mg PO/SOS
INJ HAI 4-4-4
INJ NPH 4-x-4
Vitals monitoring 4th hrly
GRBS monitoring 7th hrly
HRCT was done yesterday
Inference -
1) non resolving consolidation
2) Bronchoalveolar carcinoma
Planning for Usg guided biopsy & aspiration today
Patient was referred to higher center on 20/12/22
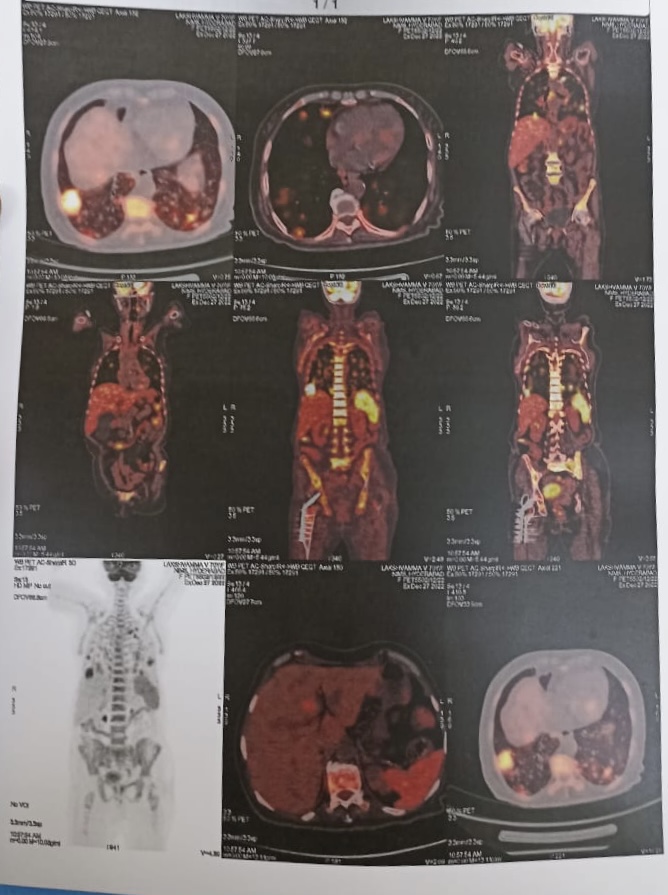
Follow up-
Upon referral patient was taken to another esteemed hospital where the necessary investigations were done and these are the reports: